

Written By Errin Lawrence – Clinical Fellow
Peer reviewed by Dr Jonny Wilkinson
What are E-cigarettes and how do they work?
Smoking-proxy electronic inhaling systems or e-cigarettes are battery-powered nicotine or non-nicotine delivery systems. They have three major component parts, a lithium battery, a vaporisation chamber and a cartridge or refillable well. The cartridge contains the ‘e-juice’, which is the liquid that contains the nicotine, the carriers for the nicotine; vegetable glycerol and propylene glycol along with associated flavourings. This is then heated in the vaporisation chamber with a heater coil, powered by the lithium battery and a vapour or aerosol is produced which the user then inhales.

The popularity and use of these products are increasing and are a multimillion-pound industry, with lacking data on the potential impact on human health in the short, or long term. The concerns that people have regarding these devices include nicotine exposure, second-hand exposure, the potential as a gateway to cigarette use/normalisation of cigarette use and the impact of the chemical compounds themselves on health.
The pro’s and not so pro’s…who is telling the truth?!!
To be honest, buried in amongst ridiculous conflicts of interest, the proponents of vaping can spout about it until the mist settles! But…what do we believe, what is recent, what is evidence-based?
What are the chemical substances contained in E-cigs…what isn’t?!
One of the most commonly known compounds receiving a lot of press is Diacetyl. The reason for this is due to the workers at a microwave popcorn processing plant reporting to hospitals with severe shortness of breath, later to be diagnosed with severe bronchiolitis obliterans. Diacetyl is a small volatile flavouring compound used for its ‘butter flavour’ in a number of foodstuffs and its effect on lung damage has been shown to be dose-dependent. It is worth noting that since 2016 under the EU Tobacco Products Directive (TPD), the use of diacetyl has been banned in e-cigarette products sold in the UK. However, this directive only covers those products that contain nicotine.
The guidance for substances that are not permitted in E–liquids, as per the TPD, can be found below:
- any ingredient that poses a risk to human health in the heated or unheated form
- vitamins or other additives that create the impression that a tobacco product has a health benefit or presents reduced health risks
- caffeine or taurine or other additives and stimulant compounds that are associated with energy and vitality;
- additives having colouring properties for emissions;
- additives that have carcinogenic, mutagenic or reprotoxic (CMR) properties in unburnt form.
From national standards:
- Substances classified as carcinogenic, mutagenic or reprotoxic (CMR categories 3, 1 and 2)
- Substances classified with specific target organ toxicity for the respiratory tract (STOT category3 1)
- Respiratory sensitizers
- Vitamins used as food supplements
- Stimulant additives such as caffeine or taurine
- Diacetyl
- Pentane 2,3 dione
- Diethylene glycol
- Ethylene glycol
- Formaldehyde*
- Acetaldehyde*
- Acrolein*Metals, including cadmium, chromium, iron, lead, mercury and nickel
- Preservatives are liable to release formaldehyde.
There is the obvious exposure to nicotine, but in addition, there is a myriad of other compounds found within the vapour.


Particles
There is no safe level of particulate matter, and although the levels in e-cigarettes are generally lower than conventional cigarettes, there is no governed safe level of particulate matter. Particulate matter smaller than 2.5 microns can be deposited in the lung and cause damage, not only this but potentially to the heart. There have also been no conclusive studies regarding the deposition of particles once they enter the moist environment of the airways. Added to all of this, different flavours have differing particles contained within.
Carbonyls
This group of compounds includes acrolein (irritant to face, eyes and nasal passages), Formaldehyde (carcinogen group 1), and acetaldehyde (carcinogen group 2b). These compounds have been found in e-cigarettes without nicotine. Formaldehyde has been noted to be present at either the same or higher levels compared to tobacco cigarettes. The level of formaldehyde found also depends on the voltage of the device used and how long the person has been vaping for.
Volatile organic compounds
This group includes benzene (carcinogenic, group 1), styrene, ethylbenzene (group 2B carcinogens), and toluene. Long term exposure to these compounds can cause damage to the central nervous system, kidneys and liver.
Heavy Metals
Heavy metals including lead, nickel, tin, chromium and aluminium have all been found in e-cigarettes, at levels equal to or higher than conventional smoking.
Glycol
Glycol is one of the main carriers within the liquids used for vaping. Although it has been tested as safe for human consumption (orally), it has not been tested for inhalation over a prolonged period of time in a situation such as vaping. Baring in mind, the surface area of the lung is different from the digestive tract, so absorption profiles will be different from this route. Glycol has been used for many years as a component in fogging liquids used in the theatres and nightclubs. There have been studies demonstrating decreased lung function amongst those exposed to them.
Microbial contamination
Lee et al looked at the level of contamination of e-liquids with endotoxin (the cell wall of gram-negative bacteria) and (1-3) Beta D Glutan (fungal cell wall). Exposure to these compounds has been linked to airflow obstruction, atopic and non-atopic asthma, as well as emphysematous changes. E-cigarettes with wicks derived from cotton fibres are particular culprits for this, as endotoxins are a natural contaminant.

So why are people doing this to themselves?!
The WHO has released quite a detailed document on the whole thing here:

At a cellular level
The table below summarises some of the cellular effects of many vape compounds.

There have been an array of studies looking at the effects of the e-juice on various cell lines in vitro. One study that used normal human bronchial cells and an air-water interface to mimic the conditions of the lung found that diacetyl and 2,3-pentanedione induced significant transcriptomic changes which resulted in a significant decrease in the number of ciliated cells in the population. T. R Rowel et al looked at 13 different flavours and compared them with a PG/VG equivalent mixture and a control. They found dose-dependent decreases in cell viability and proliferation with exposure to e-juice. Interestingly, they found that when they exposed cells to the aerosolised liquid, the results were comparable to that of the juice before it had been vaporised. They found that some flavours were more harmful than others and that high wattage of vaporiser resulted in an increase in toxic compounds.
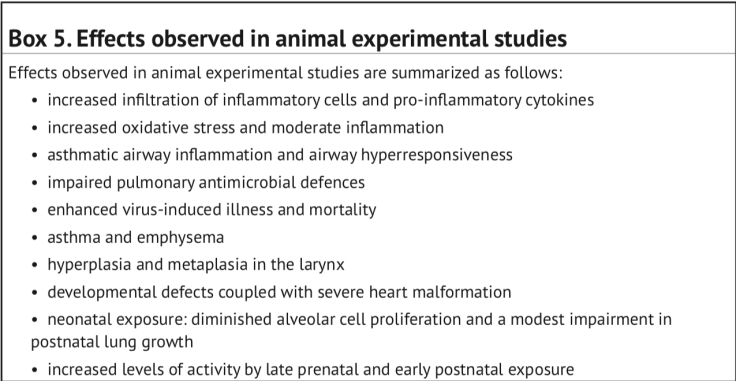
A study looking at 20 smokers and 20 non-smokers have found that there was an increase in the markers of platelet activation and platelet aggregation following the use of e-cigarettes in non-smokers and an increase in the platelet aggregation of smokers as the platelet activation levels were already raised. These effects occurred within 5 minutes of using 9 puffs of an e-cigarette The box below, again from the WHO review summarises many of the other adverse systemic effects of vapes.


Animal studies
And there always are! M.C. Madison et al looked at chronic cigarette exposure and electronic cigarette vapour exposure in mice over 4 months. They found that vapour altered the lipids in alveolar type 2 pneumocytes and macrophages, with the macrophages having increased lipid accumulation independent of nicotine and the alveolar cells having irregular unorganised lamellar bodies. Vapour exposure disrupted both the protein and lipid component of pulmonary surfactant, resulting in increased pools of surfactant in the terminal airways. Such accumulation altered normal physiological function to the point where gas exchange was affected. Interestingly, they found that as a result of the alterations, mice exposed to the flu virus had a significantly delayed response to the infection and had persistent lung inflammation independent of the nicotine concentration.
With regards to the surgical implications of wound healing a e-cigarettes, Troiano et al performed a study in rats and demonstrated that both smoking and vaping had an equally detrimental effect on flap viability. Suggesting therefore that vaping is equally as problematic in terms of wound healing post-surgery.

Human studies
J.E.Latden et al have found 53 cases of confirmed or probable pulmonary disease secondary to e-cigarette use in patients 14-30 years of age. The majority of patients had no past medical history other than asthma, and there was a mixture of rural and urban residence. The patients presented with a mixture of constitutional, respiratory and gastrointestinal symptoms, however, 98% had respiratory symptoms at the time of presentation to hospital with cough, shortness of breath and chest pain the most common. On Bronchoalveolar-lavage there were lipid laden macrophages, on the three patients who underwent a lung biopsy there was “mild and nonspecific inflammation, acute diffuse alveolar damage and foamy macrophages, and interstitial and peribronchiolar granulomatous pneumonitis”.

91% had an abnormal Chest x-ray, 48 of the 53 cases underwent a chest CT which revealed ground-glass opacity in 100% of patients.


Davidson et al reported 5 patients aged between 18-35, between July and August 2019, who presented with acute lung injury likely secondary to e-cigarette use. All of the patients had been using marijuana oils or concentrates in their e-cigarettes, all 5 were hospitalised, three required intensive care admission for acute respiratory distress syndrome and one was intubated and mechanically ventilated. CT in these cases also revealed ground-glass opacities, gain lavage cytology shows lipid within alveolar cells. A similar picture seen in the animal studies.
The Centre for Disease Control is currently investigating 805 lung injury cases and 12 deaths as a result of vaping across 46 states and one US territory. 62% of the patients are 18-34 and 69% are male. 77% reported using THC-containing products, 57% used nicotine-containing products and 16% used nicotine-containing products exclusively. All of the patients have a reported history of e-cigarette use and no consistent evidence of infection.
They have formulated a case definition for confirmed and probable e-cigarette associated lung disease.

The number of cases the CDC are investigating increases on a weekly basis and their website is updated with new cases every Thursday. Their current advice is that people should refrain from using these devices.


Their current advice for the management of the above issue is as follows:
Clinical History taking:
- Ask patients admitted to hospital with respiratory symptoms about e-cigarette use in the preceding 90 days and if suspected as a cause of this illness specifics about the type and duration of use as well as the content of the fluids used.
- IF patients admitted for other medical problems are admitted and use e-cigarettes, ask them about any respiratory symptoms.
Exclusion:
- Ensure that all other causes have been excluded such as infection, rheumatological, malignancy and immunodeficiency.
- Consider Bronchoalveolar lavage and staining of the fluid with Oil red O or Sudan Black to look for lipid deposition that is a common theme amongst the cases so far.
- Corticosteroids have been shown to be of some use in patients with lung pathology secondary to vaping.
There have been a few cases reported of poor post-operative surgical outcomes possibly related to vaping. M. Fracol et al reported a case of 51-year-old ex-smoker with a 25 pack-year history of smoking, followed by a 3-month history of vaping, which she neglected to mention to the surgeons as she did not class it like smoking. She underwent a bilateral mastectomy and insertion of tissue expanders, as part of her treatment for breast cancer. Postoperatively she suffered from tissue necrosis and had to undergo removal of the tissue expanders, debridement and closure 2 weeks post-op.

Conclusion
In conclusion, e-cigarettes are becoming more and more popular and are portrayed as a seemingly benign alternative to tobacco products. More worryingly, vaping has become extremely popular amongst adolescents, both via poor media and peer pressure. The devices are available in a myriad of forms and the fluids are sold everywhere. Where there is a convenience store, there will be 2 vaping shops! There is a multitude of manufacturers, both commercial and small scale; all vary what is contained in the liquids…smiling death dressed as sweet-smelling fluids. It cannot and simply, is not, normal to inhale oils, liquids, chemicals like this in the quantities people do! Just talk to someone who has to clean the windows in a house where someone vapes, or even worse, to car cleaners chiselling their way through the oily, dirty slime on the car windows of a vaper! The common theme is that even the inhalation of propylene glycol and vegetable glycerine carriers in themselves have an adverse effect on the lung, despite being fit for human consumption. The various flavours have health concerns in particular Diacetyl but also a number of other compounds as detailed above. Who knows what they do in combination!? There is evidence on a cellular and an in vivo level that whilst it does not carry the same risk of emphysema and carcinogenesis as cigarette smoking it is not without clearly significant and as yet unquantified risks of its own. The final thing to say is we probably have no true idea of the health impact these are having, as patients when asked if they smoke, will say no. Therefore any pathologies we see won’t be associated. But perhaps the new question should be, ‘Do you vape”?. We are going to see more and more bronchiolitis as time progresses and we may even reach a stage where these are banned! Watch this space…































Leave a Reply